This story was published in partnership with Prison Journalism Project, a national nonprofit organization which trains incarcerated writers in journalism and publishes their work. Sign up for PJP’s newsletter, or follow them on Instagram and X.
No one who knows me from the free world would ever believe that I resorted to using heroin.
I was never a party animal, and I didn’t need to use drugs to enhance my natural good vibes. It’s like the old heads used to say about getting high off of dope, “One time is too many, and too many is never enough.”
I had zero history of heroin or opioid use prior to my arrest in 2004. Many of my incarcerated peers have turned to Allah or Christ to sustain their mental and emotional health throughout our decades of incarceration. I, not being the most spiritually inclined brother, turned instead to drugs to numb the pain of my regrets stemming from my criminal activities. I did it to maintain my sanity.
Slipping into darkness, in a moment of stupidity, I started blowing joint (snorting heroin) in the DC Jail back in 2005. For a while, it worked miracles, silencing the shame and guilt I felt from the hurt I caused myself.
The drugs muzzled all the negative barking in my head: “You sold your family out for the streets. You’re a deadbeat dad. You’re an ignorant, stupid, worthless Black motherfucker. You ain’t never getting out of prison, and you deserve to die in jail.”
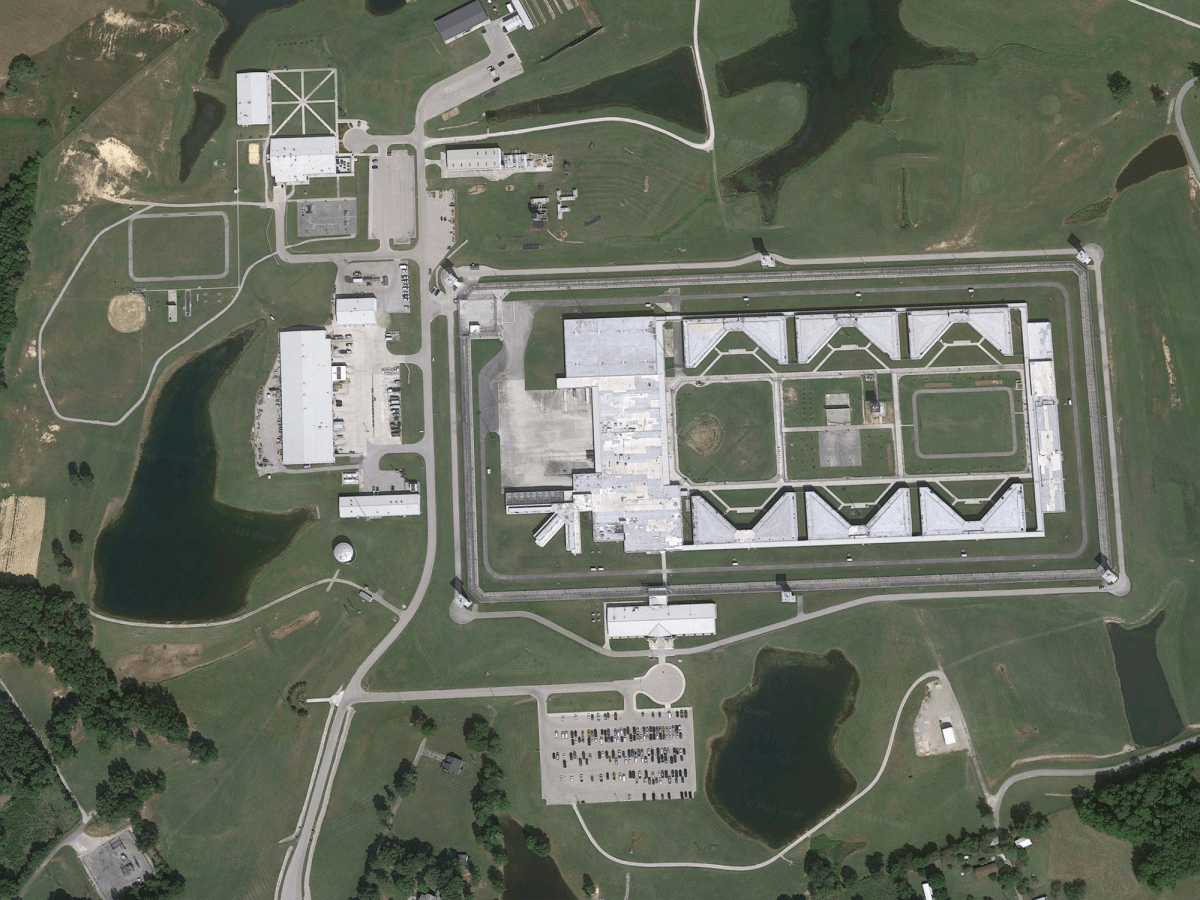
Fast forward several years. I was transferred to the Federal Bureau of Prisons to serve out my sentence, as are all people convicted of D.C. crimes. By then, those moments of euphoric escape transformed into a merciless stranglehold, a chemical and physical addiction. I still struggle to completely escape its grasp. Many of my fellow prisoners are struggling, too. And from where I’m now sitting, inside the 5A housing unit at USP McCreary in Pine Knot, Kentucky, it looks like the BOP doesn’t give a damn.
Over the past several years, there have been a slew of drug overdoses throughout BOP facilities. Too many have ended in death. Many could have been prevented.
A February report from the U.S. Department of Justice’s inspector general on deaths inside BOP facilities found that at least 70 people died of drug overdoses between fiscal years 2014 and 2021. That figure makes up about 20 percent of the 344 deaths in BOP facilities during that time. Drug overdose was the second leading cause of death; hanging was the first.
The inspector general also found “significant shortcomings” in the BOP’s responses to nearly half of all in-custody deaths the agency looked at. Problems included a lack of urgency, failure to bring the appropriate medical equipment, and issues or failure to use naloxone, the opioid overdose antidote.
The report identifies the most tragic outcomes for prisoners who are addicted to drugs, and reflects the fears of many people I know inside who struggle with opioid dependency. But the truth is that daily life for a drug-addled person in a BOP facility is much grimmer than a sterile report can convey.
***
Violence and overdoses are tragic but predictable symptoms of drug addiction both inside and outside prison. The risk of running across a bag laced with a lethal dose of fentanyl is always there. Many people dealing with addiction on the inside go into debt and are beaten off the yard when they can’t pay. Others inflict violence to feed their addiction. I have witnessed all of this. But the difference in here is access to treatment.
“One of the most horrific and traumatizing things you can witness in prison is watching a close friend, someone you love and care about, trying to kick, cold turkey, a heroin addiction,” says Leonard Bishop, a former advisory neighborhood commissioner at the DC Jail, who is now incarcerated with me at McCreary. “It’s ugly seeing brothers going through the throes of detox. Watching many of my friends and generational peers fall victim to the addictive lust for heroin and ultimately transforming into somebody that neither of you recognize—it’s hard feeling helpless to make your buddies understand that they’re playing right into their own self-destruction.”
When a prisoner decides to try and kick his habit in the BOP, he is often met with barriers, delays, and flat-out denials. The first obstacle is getting approved for treatment.
Such lifesaving medical care is promised in the First Step Act, signed into law in 2018. I have asked how to get a prescription for medication assisted treatment, such as Suboxone. But in my experience at USP McCreary, the medical and psychology departments have provided conflicting answers to my fellow prisoners and me about which department is tasked with providing addiction treatment. Neither department can explain the criteria we must meet to be placed in a recovery program.
For example, I have been told that the program is only open to guys with 90 days left in their sentence.
Michael “Boogie Swan” Johnson, from Baltimore City and who served time in USP McCreary from 2023 to 2024, says he received a similar response.
“While I was in USP McCreary, I was denied medical treatment, and they told me they were only providing medication treatment for those 90 days to the door or less,” Johnson, who has been incarcerated since he was 18 years old, says via email. “That didn’t apply to me because I have 12 years with four to go.”
He says when he was transferred earlier this year to FCI Williamsburg, a lower security facility in South Carolina, he was immediately prescribed Suboxone, a medication used to treat opioid addiction, and he now takes one 8-milligram strip per day.
“What it does is it takes out the craving for opioids,” Johnson says via email. “So it helps me function on a day-to-day basis much better.”
BOP spokesperson Randilee Giamusso says an order to begin treatment in many BOP programs “is arranged according to projected release date, [but] services should not be withheld until someone is 90 days before release.” That wouldn’t even be enough time to complete the two residential treatment programs, which run for 12 months and 18 to 24 months, respectively, she acknowledges.
The type of medication-assisted treatment that Johnson is receiving at FCI Williamsburg should be available at any point during a person’s incarceration “depending on clinical need,” Giamusso says.
Giamusso initially told City Paper that two kinds of residential addiction treatment programs should be available at McCreary. The Challenge Program, which runs from 18 to 24 months and is specific to high-security institutions, provides treatment for drug addiction and mental illness as well as violence intervention. At McCreary, the program currently has an enrollment of 46 people, according to the BOP, according to the BOP, with a waitlist of 94 people. In response to follow-up questions, the BOP clarifies that the separate Residential Drug Treatment Program, which typically runs for nine months, is not offered at McCreary. A non-residential treatment program here currently has 35 people enrolled, according to the BOP, with a 424-person waitlist.
In light of questions regarding the denial of these programs and treatment, Giamusso says that the “FBOP will be sure to follow up and provide any necessary training or information to ensure treatment is compliant with policy at all locations, including USP McCreary.”
In 2022, the Marshall Project reported on deficiencies with the BOP’s compliance with the First Step Act’s drug treatment provisions. At the time, the outlet reported that only 10 percent of the estimated 15,000 people in BOP custody who needed opioid addiction treatment were receiving it.
By the end of October 2022, nearly four years after the First Step Act went into effect, 21 prisons offered no addiction medication, and 59 more were treating 10 or fewer people, TMP reported.
Guys who are close to release should absolutely be given treatment because of their higher chance of relapse and overdose when they’re out. But what about those of us who have been led to believe we don’t qualify for treatment? We fall deeper into the disease, made to feel as though our lives are less valuable, or worse, expendable.
***
At USP McCreary, inside the 5A housing unit where I am serving my sentence, I estimate that only about 20 prisoners, out of a total of 120 housed within the unit, are employed or hold prison work details throughout the day.
Serving time at McCreary is chronically depressing. Intellectual and artistic stimuli are practically nonexistent. When we’re not locked down, we are allowed out of our cells at 6 a.m. Healthy, able-bodied men, who could be engaged in intensive rehabilitative and reentry programming, just sit around in an overcrowded day room. They play card games or other tabletop games; some play video games on their tablets.
In an attempt to break the monotony of this all-consuming idleness, some of us turn to drug use as a coping mechanism. The high provides momentary escape. But drug use and addiction in prison have ripple effects.
Some addicts are better than others at hiding their dependency. Insulated with a little cash and a degree of hustle, a prisoner with an opioid addiction can find the means to keep their fronts up by dressing neatly, shopping at commissary regularly, and paying their debts in a timely fashion, which allows them to maintain a prison work detail without a problem.
For prisoners struggling with opioid addiction who don’t have the capital to float their habit, life can be dangerous.
Addicted prisoners run up debts small and large—anywhere from $20 to $1,500 in cases that I’ve known about—that they are unable to pay. Avoiding those consequences is, in my estimation, the No. 1 cause of prisoners’ requesting placement into protective custody, which is typically an act of desperation intended to avoid violent retribution. The inspector general’s audit broadly confirms that drug addiction and debt in prison beget violence.
The more aggressive opioid addicts resort to strong-arm tactics to get their fix. Some use homemade knives and shanks to rob jailhouse dealers. I’ve been in housing units where two or three addicted prisoners mob up, walk into the cell of the prison dealer, hold him up at knifepoint, yank his pants and boxer briefs down to his ankles, and retrieve the narcotics hidden between his cheeks.
Over the years, I’ve witnessed other acts of desperation, too.
Prisoners will make shanks and sell them to anyone willing to pay—even to opposition groups—all to fuel an addiction. Making weapons for rival gangs is like treason on the inside. If he’s discovered, he could get beat, stabbed, or both.
Guys will tell all sorts of lies to their family and loved ones, goading them out of their money so they can pay for drugs inside.
Men and women have been known to sell their bodies in exchange for drugs or the money to buy drugs. This doesn’t change for incarcerated people, but it does become more dangerous. Men and women in prison don’t have condoms for protection against contracting or spreading sexually transmitted infections.
Suicide behind these walls has also been linked with drug use. The inspector general’s findings cite BOP-producted reports on two suicidal deaths that say the individuals who took their own lives “experienced hopelessness about the inability to repay their drug debt.”
And even if a BOP prisoner is accepted into a recovery program, they risk punishment (loss of good-time credit and phone, email, and commissary privileges) if they backslide and end up with a dirty piss test. Relapse is a well-understood hallmark of addiction recovery.
I have no desire to return to my family or community addicted to heroin. I recently attempted detoxing, as I have before. Every waking second, I’m thinking about it, fighting the temptation. Guys like myself, who have jailhouse addictions, are seeking addiction medication, and since we’ve been denied at USP McCreary, some of us are spending our own money on medication that the prison should be supplying to us. I pay $25 for 1/16 of a strip of Suboxone when I can afford it. Technically, it’s considered contraband.
The BOP should provide this treatment to all who need it. No more lives need be lost for a problem that the federal prison system is capable of fixing.
Additional reporting by Mitch Ryals.
This article has been updated to clarify USP McCreary does not offer a residential drug treatment program.
Askia Afrika-Ber was born and raised in Southeast D.C. and Prince George’s County and is serving a 53-year sentence for felony murder in USP McCreary, a high-security prison in Kentucky. He published a book about life inside prison in 2024. Inside Voices is produced in collaboration with More Than Our Crimes, a nonprofit dedicated to raising the voices of people locked in federal prisons across the country.